|
|
APSC-JCS Joint Symposium |
| |
| Heart Transplantation in Asia-Pacific Region: Its Status and Tasks. |
|
| |
|
| Heart Transplantation in Australia-2009. |
| Don Esmore |
Alfred Hospital, Melbourne, Australia |
| |
Prof. Don Esmore, Alfred Hospital, Melbourne, Australia, overviewed the status of heart transplantation in Australia. More than 1,900 heart transplants have been performed in Australia since 1984, when the first transplants were performed. Currently, Australia has four adult and one pediatric heart transplant programs compared with 160 programs in the United States. Heart transplants comprise 9% of all transplants in Australia.
Mean waiting time to heart transplant peaked in 1999 at about 230 days, dropping to about 150 days in 2007. The organ donation rate for hearts in Australia is 11 per million population per year, about half that of Europe and America. The heart transplant rate in Australia is 3.5 per million population per year compared to 7.0 per million population per year in western countries. Heart transplantation in Australia is government funded.
In Australia the mean ischemic time for transplanted hearts is about 4 hours compared with 160 minutes in the ISHLT registry. Long-term survival is the same for hearts with ischemic times ranging from under 2 hours to over 6 hours. Extracorporeal membrane oxygenation (ECMO) for primary graft failure has increased in recent years to 20% of heart transplants. The reason for the increase is unknown.
|
Figure 1. Actuarial survival pre-treatment and status: 1984-2007
【Click to enlarge】 |
|
|
Mechanical circulatory support (MCS) as a bridge to transplantation (BTTx) using a ventricular assist device (VAD) has been used in Australia since the early 1990s. Approximately 25 VADs are implanted in Australia each year. The mortality rate associated with BTTx is 20% to 30%. From 2005 to 2007 about 25% of all heart transplants are performed in patients with VADs. Early post-transplant mortality is a little higher in patients with VADs probably due to the more complicated surgery (Figure 1).
Alfred Hospital has performed 26 heterotopic transplants, with 12% mortality at a median follow-up of 7 years. Indications include high pulmonary vascular resistance (PVR), older patients, blood group O, donor to recipient weight discrepancy, marginal donor, long ischemic time allografts, and re-transplants. Early mortality is high with heterotopic tranplant but 6-year survival is about 60%.
|
Figure 2. Heart transplant survival in Australia compared to the ISHLT.
【Click to enlarge】 |
|
|
Overall heart transplant mortality is lower in Australia than in the ISHLT registry, with 35% survival at 21-22 years (Figure 2).
Heart transplantation is available to all residents of Australia. There are only four adult heart transplantation programs, ensuring maximal Unit experience. Optimal use is made of available donor organs and a full spectrum of clinical options is available. Survival outcomes are better than the world average. |
| |
| Page Top |
|
| |
|
| Heart Transplantation in Korea |
| Pyowon Park |
| Department of Thoracic & Cardiovascular Surgery, Samsung Medical Center, Seoul, Korea |
| |
|
Figure 1. Annual number of heart transplants in Korea.
【Click to enlarge】 |
|
|
Dr. Pyowon Park, Samsung Medical center, discussed the status of heart transplantation in Korea. The first heart transplant in Korea was performed in 1992, with 10 to 30 performed annually through 2006 (Figure 1). In 2007, 50 transplants were performed. In 2008, the number increased to 84, possibly due to increased publicity about organ donation, more transplants performed in the elderly, use of marginal donors, change of funeral patterns from burial to cremation, and financial support for organ donation.
There are six heart transplantation centers in Korea, most located in Seoul. The cold ischemic time for donated hearts is less than 4-5 hours. Heart transplant status is defined as: Status 0 (first priority)–extracorporeal membrane oxygenation (ECMO) or ventricular assist device (VAD) with ventilator; Status 1 (second priority)–ECMO or VAD without ventilator, intra-aortic balloon pump (IABP), ventilator, or IV inotropics >4 weeks; Status 2–IV inotropics <4 weeks; Status 3–other recipients. Allocation priority for Status 2 and 3 is determined by calculating points based on several factors. The average waiting time to transplant is 27 days for Status 0, 60 days for Status 1, and 99 days for Status 2 and 3.
In 2008, 209 hearts were donated but only 74 (35%) were transplanted. The remaining 65% were not used for various reasons, including unsuitable donor heart (34%) and recipients rejecting the donor heart (25%). From 2000-2007, most heart transplants were performed in recipients aged 35-49 (37%) and 50-64 (28%). The incidence in recipients under 18 years was 18% and in those ≥65 was 3%. Males received 75% of the heart transplants.
|
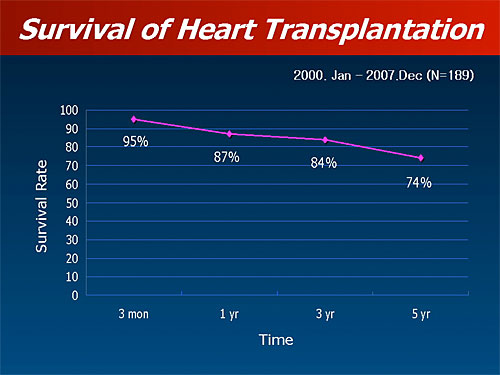
Figure 2. Survival of heart transplantation in Korea.
【Click to enlarge】 |
|
|
Currently, no long-term mechanical support devices are available for bridge to transplantation (BTTx). ECMO or centrifugal LVAD are used for short-term support. From 2000-2007, 5-year survival after heart transplantation was 74% (Figure 2).
From 1996-2009, 96 heart transplants were performed at Samsung Medical Center (SMC). The median age of recipients was 44 years. Mechanical support methods for BTTx were 14 ECMO (1 LVAD), 1 Jarvik heart (implanted in U.S.), and 4 IABP. The median ECMO support time was 201 hours. The incidence of marginal donor hearts in ECMO patients was 79% versus 47% in those without ECMO (p=0.03). In patients with ECMO, 4 had ECMO, 1 had IABP, and 6 had hemofiltration post-transplantation. The median ICU stay was 16.5 days and 3-month mortality was 29%. The overall 3-month, 5-year, and 10-year survival rates at SMC were 90%, 51%, and 43%, respectively.
|
| |
| Page Top |
|
| |
|
| A Good Prognosis for Japanese Heart Transplant Recipients – A Statement from the Japanese Circulation Society Heart Transplant Committee. |
| Kazuhiko Nishigaki |
| Second Department of Internal Medicine, Gifu University School of Medicine, Japan |
| |
Dr. Kazuhiko Nishigaki (Gifu University School of Medicine), Secretary of the Japanese Circulation Society Heart Transplant Committee, described the Transplant Committee’s study of Japanese heart transplant candidates approved for transplantation since establishment of the Organ Transplant Law in 1997. Although heart transplantation is recognized worldwide to improve outcomes for patients with severe heart failure (HF) who do not benefit from lifesaving and/or conventional therapy, only a few heart transplants are performed annually in Japan.
The purpose of the Transplant Committee’s study was to determine the prognosis of heart transplant recipients. Data were collected via a questionnaire from 524 heart transplantation applicants between April, 1997 and October, 2008. The patients outcomes were evaluated on November 1, 2008. Among the 524 applicants, 503 (96.5%) completed the questionnaire. The average age was 32 years, with 78 applicants ≤15 years. There were 365 males and 138 females, with a male to female ratio of 2.6. About 70% of applicants had dilated cardiomyopathies; 7.8% had ischemic cardiomyopathy. Of the 503 applicants, 432 (86%) passed the evaluation. Of these, 136 (31%) received a transplant, 50% in the U.S., 6% in Germany, 1% in Canada, and 43% in Japan (13.3% of all applicants).
Among the 432 patients who passed the evaluation, 254 (58.8%) were alive at the end of the study, with 125 (49.2%) of these transplanted and 129 (50.8%) not transplanted. A total of 174 (40.3%) died, 10 (5.7%) of whom were transplanted and 164 (94.3%) not transplanted. Among patients surviving without a heart transplant, 53 (41%) remained hospitalized, while 97% of transplant recipients were treated as outpatients and 83 (66%) returned to work.
|
Figure 1. The causes of death in heart transplant-acceptable patients.
【Click to enlarge】 |
|
|
|
Figure 2. Survival curves for the heart transplant-Aaceptable patients.
【Click to enlarge】 |
|
|
Among patients who qualified for heart transplantation, the main causes of death among non-recipients were HF (33%), cerebral infarction (18%), and severe infection (14%). The main causes of death among transplant recipients were chronic rejection (30%) and severe infection (30%) (Figure 1). Patients who did not receive a transplant had a 2-year survival rate of 53% and 5-year survival of 30%. Among transplant recipients, the 5-year survival rate was 90% (Figure 2).
In summary, overall 31% of applicants received a transplant. The survival rate of transplant recipients was very good, both those transplanted domestically and internationally. Dr. Nishigaki concluded that heart transplantation is the ultimate treatment to dramatically improve the prognosis of patients with severe heart failure. For the purpose of promoting heart transplantation, revision of the early organ transplant bill would be highly desirable. |
| |
| Page Top |
|
| |
|
|