 |
|
|
|
MIKAMO
Lecture
New Developments in Echocardiography: Impact
on Coronary Artery Disease |
|
Harvey Feigenbaum, M.D.
Indiana University
Indianapolis, Indiana, USA |
|
 |
|
|
|
|
|
|
The impact of new advances in transthoracic
contrast echocardiography on the diagnosis and therapy
of coronary artery disease was the subject of the invited
Mikamo Lecture delivered by Dr. Harvey Feigenbaum of Indiana
University, Indianapolis, Indiana.
Contrast echocardiography, tissue imaging,
endocardial border detection, 3-D echocardiography, and
digital echocardiography were the key developments discussed.
Harmonic imaging, intermittent imaging, power Doppler,
pulse inversion, real-time perfusion imaging, quantitation
with video densitometry and digital enhancement are also
contributing to the revolution in contrast echocardiography.
|
PAGE
TOP
|
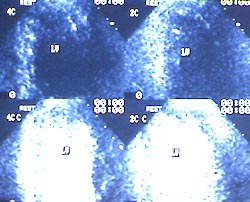 |
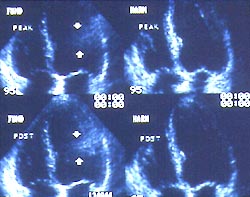
Figure
1. Echocardiograms demonstrating how intravenous
contrast can highlight the cavity of the left
ventricle and outline the myocardium. The upper
two echograms are without contrast and the lower
two echograms show the affect of the intravenous
contrast.
Click
to enlarge |
|
New contrast agents are revolutionizing clinical
echocardiography by enhancing the resulting images
(Fig. 1). An albumin-coated air microbubbles agent
was the first of these new agents, but has been
replaced by an albumin-coated fluorocarbon-based
bubbles agent that persists much longer and provides
brighter echos. Saccharide-coated fluorocarbon bubbles,
phospholipid-coated fluorocarbon bubbles, and fluorocarbon
emulsions are available among many others. A large
number of commercial bubbles will be available soon.
Agents that will better opacify the myocardium to
see whether or not there is perfusion throughout
the entire heart muscle are under development.
|
|
PAGE
TOP
Advances
in imaging of contrast agents |
|
The use of harmonic imaging, intermittent
imaging, power Doppler, and how the contrast is
analyzed are providing better images.
Harmonic imaging
Harmonic imaging is a major breakthrough.
When an ultrasonic beam interacts with a bubble
it expands and contracts and thus sends off a secondary
frequency, a harmonic frequency, usually at a multiple
of the transmitted frequency. Since bubbles oscillate
and noise and for the most part tissue do not oscillate,
the signal-to-noise ratio can be enhanced, allowing
bubbles and echo to be better distinguished.
Intermittent Imaging
Intermittent imaging of every third
or fifth cardiac cycle allows for better opacification
of the myocardium. The Doppler signal itself interacts
with the bubbles not only by oscillation but by
actually destroying the bubble. In contrast, continuous
imaging yields a very faint opacification because
the ultrasonic beam is destroying the bubbles.
Power Doppler
Power Doppler is an even more powerful
way to destroy bubbles to yield a very strong signal
to enhance the contrast effect. Power modulation,
another new technique offering great promise, hits
the heart with a very high mechanical index, 0.7,
to destroy all the bubbles. The myocardium is then
echo free, which is followed by gradual reperfusion
and bubble reaccumulation in the myocardium, allowing
time to evaluate myocardial reperfusion.
Analysis of Contrast
Video densitometry and digital enhancement
are being used to improve analysis of the contrast
agents. Investigators are attempting quantification
using video densitometry to see the change in amplitude
of the signal of the contrast agent in the perfused
area versus the nonperfused area. Kaul has shown
that digital enhancement can produce striking images.
However, this process is extremely intensive and
the reproducibility of these studies by other investigators
has been limited to date. Logistical and technical
details must be worked out, but there is great optimism
that it will be possible to reproduce such digital
images in a consistent, reliable fashion.
|
|
PAGE
TOP
Clinical
applications for contrast echocardiography |
|
Contrast echocardiography using harmonic
imaging is being used for endocardial border definition
by opacifying the left ventricular cavity. This
has been approved for clinical use in the United
States, and patients with coronary artery disease
will warrant this application.
The most intriguing application and
the one being most intensely investigated is for
myocardial perfusion. The bubbles enhance the left
ventricular cavity by passing through the right
side, passing into the left ventricle, outlining
the cavity and providing greater definition of the
septal and lateral walls. The clinical aim is to
consistently see the lack of myocardial perfusion
resulting from coronary obstruction.
Kaul has shown that harmonic imaging
of the ischemic muscle is a brighter more consistent
recording that better shows the homogeneous lack
of perfusion in the myocardium. Work from Porter
has shown the lack of perfusion when ischemia is
produced.
|
|
PAGE
TOP
|
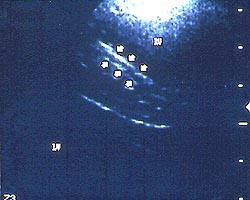 |
| Figure
2. High frequency transthoracic echocardiogram
of a segment of the left anterior descending artery
in an adult. The walls of this normal coronary
artery are thin and homogenous (arrows).
|
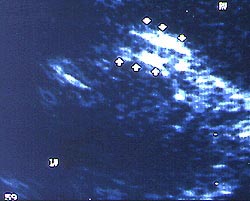 |
| Figure
3. Another high frequency transthoracic echocardiogram
of a left anterior descending coronary artery
with atherosclerosis. One can appreciate a very
thick walled vessel. The lumen is not necessarily
decreased, however, the overall diameter including
the thickened walls is dilated, i.e., remodeling.
|
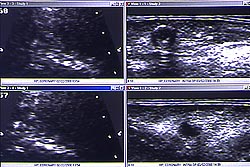 |
Figure
4. A high frequency transthoracic echocardiogram
compared with an ultra high frequency epicardial
examination of the same patient at the time of
cardiac surgery. The transthoracic echocardiograms
on the left show the "lumps and bumps" along
the walls of this left anterior descending artery.
Similar intravascular lesions are demonstrated
on the epicardial echograms on the right.
Click
to enlarge |
 |
Figure
5. Four chamber echocardiograms taken with fundamental
imaging on the left and harmonic imaging of tissue
on the right. There is a prominent artifact (arrows)
noted with fundamental imaging. This artifact
disappears with the use of harmonic imaging of
tissue. In addition, the endocardium of the lateral
wall is more readily available with this enhanced
imaging technique.
Click
to enlarge |
|
Broadband Tissue Imaging
Broadband multi-frequency transducers
with a lower frequency that provides better penetration
and a higher frequency that improves resolution
are becoming standard. Replacing lower power transducers
are 4-2 MHz broadband transducer, 7-4 MHz or an
11-8 MHz transducer.
Coronary artery visualization is being
actively investigated. The left anterior descending
is viewed transthoracically as a sample site of
the coronary circulation based on the assumption
that coronary artery disease is a diffuse process.
Figures 2 to 4 demonstrate the utility of high frequency
imaging. This technique is being developed to noninvasively
detect subclinical coronary atherosclerosis to better
define which patients should be treated with lipid
lowering agents, statins, and aspirin.
Harmonic Tissue Imaging
Harmonic imaging of tissue clearly
enhances endocardial and myocardial visualization
(Fig. 5), and is available on virtually every instrument
today. Tissue produces a harmonic signal and by
sampling the signal returning from tissue a greater
signal-to-noise ratio is achieved. Harmonic imaging
of tissue requires a high mechanical index, whereas
harmonic imaging of bubbles requires a low index.
However, because this method can make things appear
thicker, such as valves, it is necessary to consider
this when viewing harmonic tissue images. This technique
has become a standard way of doing most stress echocardiograms
in most laboratories.
Tissue Doppler
Tissue Doppler can be used to quantitate
wall motion, look at various parts of the heart,
assess systolic and diastolic function as well as
examine the mitral annulus for diastolic function.
The concept of myocardial strain to improve quantitating
myocardial contraction, and a variety of other ways
to quantify ventricular function are also being
investigated. The ability to automatically track
the color Doppler to measure flow by measuring the
diameter and the velocity is being developed. These
developments will provide more direct myocardial
indicators, rather than the hemodynamic indicators
presently used.
The amplitude of motion of the annulus
is a very important prognostic indicator of left
ventricular function as shown by a 1997 study using
M-mode echocardiography. In people with heart failure
over age 65 years with an amplitude of the annulus
greater than 10 mm, the one year mortality was zero.
However, if the amplitude was less than 6 mm, there
was about a 35% risk of mortality. Recording the
motion using tissue Doppler of the annulus combined
with the mitral flow allows for improved evaluation
of the hemodynamics and myocardial function.
Tissue Doppler has been used for the
differentiation of restrictive cardiomyopathy and
constrictive pericarditis. Any condition that restricts
the myocardium will cause abnormal annulus motion
with a short E and a tall A. But in the case of
a pericardial problem and a normal myocardium, the
annular motion is normal because of the normal myocardium.
Work from Garcia shows that the resting systolic
velocity, roughly 10 cm/second, increases to about
30-40 cm/second with dobutamine in normal myocardium.
But, if ischemia is present there is no increase
in velocity in response to dobutamine.
Automated quantitation will be the
likely result of improved endocardial border definition.
This could be done on-line on the ultrasound instrument
or off-line on a computer. The improved definition
of the endocardium needed for on-line measurements
will come from harmonic tissue imaging and the new
contrast agents.
|
|
PAGE
TOP
|
3-D echocardiography is an area of
active investigation and has been used in valvular
and congenital heart diseases. Potential applications
are assessing left ventricular volumes, which will
clearly be more accurate than 2-D, and for stress
echo.
Parallel processing is an important
technique. A limitation of ultrasound is the fact
that sound moves slowly. Parallel processing samples
one signal multiple times. One technique samples
the signal 16 times, effectively increasing the
speed by a factor of 16, with the goal of producing
real-time 3-D echo. A prototype instrument for parallel
processing is producing some very interesting and
encouraging work. Real-time 3-D echocardiography
will be a reality, and it will have a major impact
on cardiac ultrasound.
Handheld Echocardiographs
Small handheld echographs being developed
will provide the ability to put a transducer on
a patient's chest at the bedside to actually see
inside the heart and obtain either a color or black
and white 2-D echocardiogram. This will have a major
impact on the use of cardiac ultrasound. A former
president of the American College of Cardiology,
Dr. Richard Popp, wrote in a 1998 article that the
physical examination of the future will include
echocardiography as part of the assessment.
|
|
PAGE
TOP
|
The reliance on analogue videotape
in echocardiography has many limitations. Digital
echocardiography offers manipulation and display
of images not possible with videotape. The ability
to view serial studies as well as resting and stress
images side-by-side simultaneously is a clear advance.
In the setting of coronary artery disease this ability
is critical, and in acute myocardial infarction
there is improved ability to assess changes in global
or regional ventricular function over time. Regional
dysfunction is more easily judged with digital echo,
and some subtle wall motion abnormalities are best
detected with digital echo. Wall motion may be delayed,
or the abnormality may occur in diastole rather
than systole and is not apparent in real-time imaging.
Frame-by-frame or partial cardiac cycle analysis
is an advantage when assessing wall motion. Simultaneous
viewing of the digital echo and the coronary cineangiogram
is a clear advantage.
All ultrasound instruments today have
digital output. New software packages permit using
the digital output in a convenient, simple fashion.
Digital echo is the best technique to look at the
damaged myocardial muscle as it best defines the
infarct damage. Other complications, such as mitral
insufficiency, can be seen in 10-15 seconds at the
bedside with digital technology, whereas with videotape
10-15 minutes would be required.
|
|
PAGE
TOP
Report
Index | Previous Report | Next
Report
Scientific
Sessions | Activities
| Publications
Index
Copyright © 2000
Japanese Circulation Society
All Rights Reserved.
webmaster@j-circ.or.jp
|
|