|
|
ACC/JCS Joint Symposium |
| |
| Topics in the Treatment of Severe Heart Failure |
|
| |
|
| Cardiac Resynchronization and Cardiac Remodeling in Advanced Heart Failure |
| Martin G. St. John Sutton |
| Hospital of the University of Pennsylvania |
| Pennsylvania, USA |
| |
Pharmacologic treatment of heart failure attenuates left ventricular (LV) remodeling, while cardiac resynchronization therapy (CRT) may actually reverse remodeling. Dr. Martin G. St. John Sutton, University of Pennsylvania, reviewed results of CRT trials in patients with advanced heart failure.
CRT has been limited to patients with NYHA symptom class III/IV systolic congestive heart failure (CHF), QRS duration >120 ms (30-35% of patients), LV ejection fraction (LVEF) <35%, cardiomegaly >55 mm at end-diastole, and who have received optimal medical therapy for more than one month. In all the CRT trials to date, 60% to 70% of patients experienced symptomatic benefits, including improved quality of life (QOL), New York Heart Association (NYHA) symptom class, exercise capacity, and peak VO2. The MIRACLE study demonstrated that the benefits of CRT are sustained for at least two years. The symptomatic benefits of CRT are accompanied by the structural changes associated with reverse remodeling, including reduced LV volume, improved LVEF, normalized LV cavity shape, normalized mitral valve geometry, and decreased severity of mitral regurgitation. The COMPANION and CARE-HF trials demonstrated significant improvements with CRT compared to medical therapy.
CRT reduces or reverses dyssynchrony in patients with heart failure. Patients without dyssynchrony do not benefit from CRT. Other mechanisms associated with response to CRT are time to peak regional myocardial velocity, regional displacement, strain and strain rate, timing of regional end-systolic volumes, reduced inter- and intra-ventricular conduction, and decreased severity of mitral regurgitation. Tissue Doppler imaging (TDI) can detect myocardial dyssynchrony before implantation of devices and may predict optimal response to CRT).
Three recent trials have provided important information about CRT and ventricular remodeling. The RETHINQ trial reported that CRT was not effective in patients with a narrow QRS (<120 ms). The PROSPECT trial found that no single echocardiogram/Doppler measure predicts response to CRT. The REVERSE trial studied the efficacy of CRT in patients with NYHA symptom class I and II heart failure but the results had not been released at the time of this presentation.
Dr. Sutton concluded that QRS duration does not correlate with response to CRT. Patients with QRS <120 ms derive little symptomatic benefit from CRT because they do not exhibit reverse remodeling. He presented a stepwise illustration of the use of CRT as a treatment option for CHF. |
| |
| Page Top |
|
| |
|
| Cardiac Transplantation in the United States |
| Jon A. Kobashigawa, MD |
| David Geffen School of Medicine at UCLA |
| Los Angeles, California, USA |
| |
Survival, rejection, and cardiac allograft vasculopathy (CAV) rates in cardiac transplant patients have improved in the United States over the last decade. Dr. Jon A. Kobashigawa, David Geffen School of Medicine at UCLA, reviewed the latest advances in cardiac transplantation, including new noninvasive methods for immune monitoring.
Current immunosuppressive regimens consist of either tacrolimus or cyclosporine plus mycophenolate mofetil (MMF), sirolimus, or azathioprine, usually with prednisone. The decline in rejection rates most likely is due to use of the newer immunosuppressive agents (MMF, tacrolimus, sirolimus). A randomized trial by Dr. Kobashigawa found that patients treated with tacrolimus and MMF had fewer rejections and improved side effect profiles compared with patients treated with cyclosporine and MMF or tacrolimus and sirolimus.
CAV is a major factor limiting long-term survival after cardiac transplantation. Detection of CAV has improved with the use of intravascular ultrasound (IVUS). A study of 5-year outcomes in patients who had two IVUS examinations at 4-6 weeks and 1 year after transplantation validated the use of IVUS as a surrogate marker for 5-year outcomes. The study found that patients with first-year change in maximal intimal thickness (MIT) ≥0.5 mm had a higher incidence of death or graft loss, more major adverse cardiac events, and more newly occurring angiographic luminal irregularities than patients with MIT <0.5 mm.
|
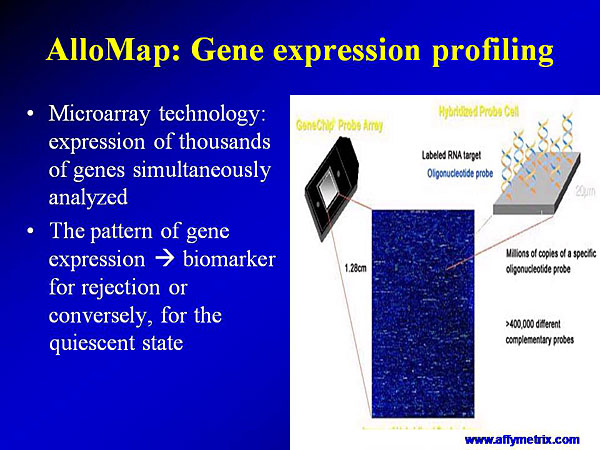
Figure 1: Process for gene expression profiling with MicroAssay technology.
【Click to enlarge】 |
|
|
|
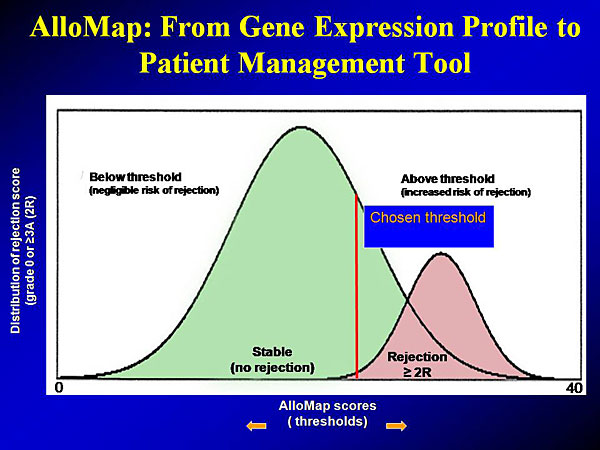
Figure 2: AlloMap: From gene expression profile to patient management tool.
【Click to enlarge】 |
|
|
Two new tests, ImmuKnow and AlloMap, provide noninvasive monitoring of transplant recipients’ immune status. ImmuKnow results reflect the degree of a recipient’s immunoresponsive state and risk for rejection and infection. ImmuKnow evaluates CD4 T cell function by measuring the amount of ATP produced by activated CD4 cells derived from a patient’s peripheral blood lymphocytes. ATP >525 ng/mL indicates a strong immune response (not immunosuppressed), while ATP <225 ng/mL indicates a weak immune response and probable over-immunosuppression. In a study of 504 transplant recipients, stable recipients with ATP=280 ng/mL had a 96% negative predictive value (NPV) for rejection and infection.
AlloMap is a peripheral blood gene expression test with a high negative predictive value to rule out cellular rejection. Using microarray technology to analyze thousands of genes (Figure 1), AlloMap has yielded a pattern of gene expression that can be used as a “fingerprint” of rejection or quiescence (Figure 2).
Dr. Kobashigawa concluded that immune monitoring tests appear to be reliable and may be helpful in cases where biopsy is equivocal. However, more clinical studies are needed prior to replacing the endomyocardial biopsy with these noninvasive tests in heart transplant recipients. |
| |
| Page Top |
|
| |
|
| Percutaneous Intervention in Left Ventricular Dysfunction |
| Liliana Grinfeld, MD |
| Hospital Italiano |
| Buenos Aires, Argentina |
| |
Coronary artery disease is the leading cause of heart failure, which is increasing in incidence and prevalence worldwide. Dr. Liliana Grinfeld, Hospital Italiano, Buenos Aires, Argentina, reviewed recent and current studies of revascularization procedures in patients with heart failure.
Among patients who have acute myocardial infarction (MI), 22% of men and 46% of women will be disabled with heart failure within 6 years. About 70% of patients with heart failure have coronary artery disease. Studies have shown that 5-year survival is superior in heart failure patients treated with coronary artery bypass graft (CABG) than in those who received medical treatment. Patients with the worst left ventricular (LV) function had the greatest benefit from revascularization.
|
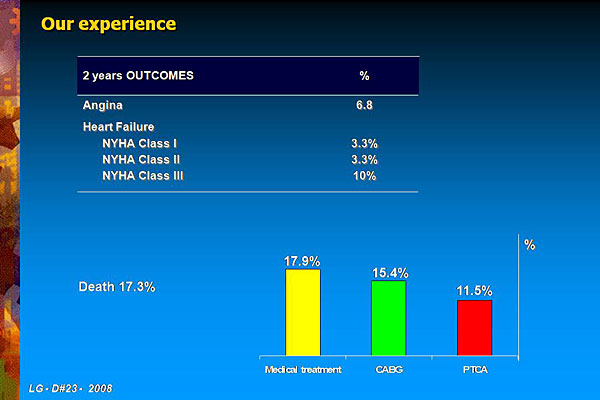
Figure 1. Two-year outcomes in the 382 patients in the STICH registry from Grinfeld’s hospital.
【Click to enlarge】 |
|
|
|
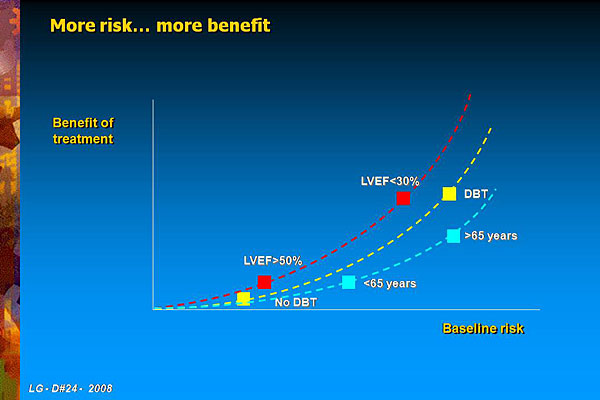
Figure 2. Two-year data from the STICH registry of Grinfeld’s patients show that the persons at greatest baseline risk derived the greatest benefit from surgical revascularization, including patients with LVEF <30, diabetes, or who are older than 65 years.
【Click to enlarge】 |
|
|
|
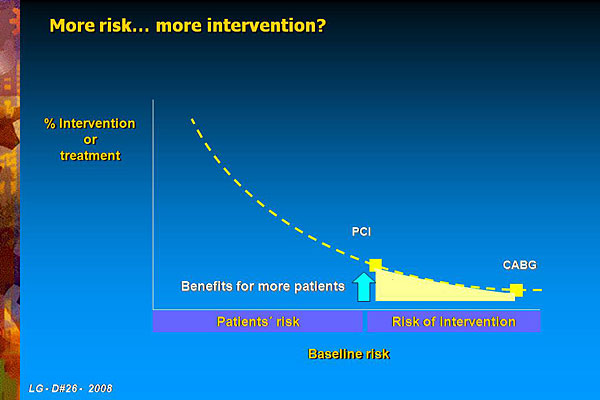
Figure 3. As risk rises, the rate of intervention decreases, as shown by the STICH registry data.
【Click to enlarge】 |
|
|
The AWESOME and REHEAT studies comparing CABG and percutaneous coronary intervention (PCI) in patients with LV dysfunction found that both procedures equally improved LVEF. A study in patients with LV dysfunction reported fewer cardiovascular deaths (P=0.05) and major adverse cardiac events (P=0.003) in patients revascularized with drug eluting stent (DES) using sirolimus versus bare metal stent (BMS).
Even though the evidence shows that survival is better with revascularization, a Duke University study showed that most patients with LV dysfunction receive medical treatment (71%) compared with CABG (22%) and PCI (7%).
Dr. Grinfeld is involved in the ongoing Surgical Treatment of Ischemic Heart Failure (STICH) registry study of surgical revascularization in 382 consecutive patients with coronary artery disease and LV dysfunction. At baseline, 24.9% of patients had previous CABG and 11.0% had prior percutaneous transluminal coronary angioplasty (PTCA). After two years follow-up, 83% of the patients had received medical treatment, 10.2% received CABG, and 6.8% received PTCA. At two years, angina was reported in 6.8% of patients, heart failure in 16.6% of patients, and death in 17.3% of patients (Figure 1). Among those who died, 17.9% had medical treatment, 15.4% had CABG, and 11.5% had PTCA.
Dr. Grinfeld concluded that the patients who derive the greatest benefit from surgical revascularization are those with the greatest baseline risk, including patients with LVEF <30, diabetes, or who are older than 65 years (Figure 2). However, most high risk patients are not receiving interventions. The best strategy for these patients probably is to choose PCI or CABG based on the patient’s baseline risk and the intervention risk (Figure 3). The potential benefits from revascularization must be weighed against high periprocedural risks. PCI may offer a safer profile than CABG.
|
| |
| Page Top |
|
| |
|
|