| Diastology is defined as a new science and art of medicine devoted to the study
of the diastolic phase of the cardiac cycle, extending from the genes to the
population in health and in disease states. |
|
| Diastolic heart failure
occurs (DHF) as frequently as systolic heart failure
(SHF), according to data from the Framingham Heart Study
showing a 50% incidence of DHF. Data from Olmstead County
(population 100,000; location of Mayo Clinic) showed
a 43% incidence. The Cardiovascular Health Study and
the Strong Heart Study, both in the United States, show
a greater incidence for DHF at 55% and 53% respectively
than SHF. Older persons comprise the majority of patients
in this new epidemic, with the incidence of DHF and
SHF increasing quite rapidly after age 60 years. In
persons over age 70 years, both the prevalence and mortality
of DHF is 50%; the mean age is 75 years. DHF is predominant
after age 90 years. |
PAGE
TOP
|
Pathophysiologic Basis of DHF |
|
The natural history of DHF begins with normal myocardium,
then hypertrophied myocardial cells producing abnormal
relaxation, and then further progression resulting
in interstitial fibrosis and increased collagen and
finally development of mild compliance abnormalities.
Calcineurin activation and angiotensin II contribute
to the formation of myocardial hypertrophy and fibrosis.
Calcium plays a critical role in the natural history.
When calcium interacts with troponin C, it results
in a transfiguration of the tropomycin-troponin complex
and opens binding sites. Calcium attaches to troponin
C, binding sites are activated, contraction, relaxation,
and then filling occurs. In the normal cardiomyocyte
the calcium transient goes through the cycle and then
disappears. Abnormal calcium homeostasis results in
abnormal relaxation.
|
PAGE
TOP
|
|
Diastolic function is a complex sequence of multiple
interrelated events: relaxation, suction, erectile
coronary effect, viscoelastic forces, pericardial
restraint, ventricular interaction, atrial contraction,
chamber stiffness and myocardial stress/strain relations.
Diastolic dysfunction is an abnormality of one or
more of these events. In simplified terms, the major
determinants of left ventricular (LV) filling are
elastic recoil (suction); myocardial relaxation (Tau);
LV chamber compliance, left atrial pressure and heart
rate.
Systemic hypertension is the major cause of DHF
and is seen in 70% of patients with this dysfunction.
Other conditions that contribute to DHF, alone or
in combination with hypertension, are left ventricular
hypertrophy, ischemic heart disease (IHD), diabetic
disease, and valvular heart disease. Less common contributors
are restrictive cardiomyopathy, constrictive pericarditis,
hypertrophic cardiomyopathy, infiltrative disorders
such as amyloid heart disease, storage disorders,
and obstructive sleep apnea. Obesity, older age and
female gender predispose to development of DHF.
|
PAGE
TOP
|
Recognition of Diastolic Heart Failure |
|
DHF is clinically indistinguishable from SHF based
on history, physical examination, ECG and chest x-ray.
Even elevation of BNP, now often used for diagnosing
CHF, does not distinguish between the two forms of
dysfunction. At least one study has shown that the
most marked elevation of BNP occurs in patients with
both.
To diagnose DHF, abnormal relaxation, filling or
stiffness must be demonstrated, in addition to clinical
symptoms and the presence of normal elevated systolic
function. According to the Framingham Heart Study,
a definitive diagnosis requires the presence of heart
failure with a normal ejection fraction noted within
72 hours of admission and, importantly, a cardiac
catheterization to establish high filling pressures.
Probable or possible DHF is diagnosed in the presence
of these features and the absence of a cardiac catheterization.
However, the requirement of a cardiac catheterization
renders this definition impractical.
|
 |
| Figure
1. |
|
The ACC/AHA guidelines state that the diagnostic
evaluation for heart failure should include parameters
to determine the type and severity of cardiac dysfunction,
determine prognosis, and guide treatment. The guidelines
recommend Doppler to assess systolic, but more importantly
diastolic dysfunction.
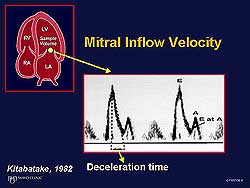
Pulse Doppler techniques provide the ability to study
the LV during diastole in health and disease and hence
provide a non-invasive method to study DHF. Parameters
that can be evaluated with Doppler are listed in Figure
1. Mitral inflow velocities (Figure 2), pulmonary
venous flow and Doppler tissue imaging are the three
most important parameters. Three patterns of diastolic
cardiac dysfunction have been established: normal,
abnormal relaxation, and restrictive pattern.
|
PAGE
TOP
|
 |
| Figure
3. Representative measurement of Grade I and Grade
III diastolic dysfunction. |
| Click
to enlarge |
|
Grade One DHF: mild diastolic dysfunction, abnormal
relaxation, earliest abnormality. Grade Two: intermediate
degree of diastolic dysfunction. Grade Three: advanced
diastolic dysfunction with high filling pressures,
restrictive pattern. Grade Four: advanced heart failure
that remains constrictive despite treatment; poor
prognosis. The filling patterns correlate with filling
pressures. Grade One diastolic dysfunction nearly
always has normal resting mean left atrial pressure.
In contrast, Grade Three diastolic dysfunction pattern
always implies markedly elevated mean left atrial
pressure (Figure 3).
|
PAGE
TOP
|
|
Doppler tissue imaging is a reliable, easy and reproducible
methodology. Advancing degrees of diastolic dysfunction
are associated with changes in the mitral E and A
velocities. But, these are discordant changes. On
tissue Doppler at the mitral level, the E prime velocity
remains reduced with advancing diastolic dysfunction.
As the disease progresses and filling pressures increase,
the mitral E and the annulus E velocities increase,
thus increasing their ratio. Thus, the ratio of mitral
E to annulus E velocity is informative.
|
PAGE
TOP
|
Constrictive
Pericarditis |
|
The E to E prime ratio and the mean left atrial pressure
is increased in patients with elevated diastolic pressures,
according to data from the Mayo Clinic, and in other
heart diseases, except constrictive pericarditis.
In this setting, as the ratio increases, the mean
left atrial pressure is decreased, resulting in a
paradox in which high pressures correlate with a low
ratio since the E prime is well preserved.
|
PAGE
TOP
|
Pulmonary
Venous Flow Pattern Interrogation |
|
A reduction in the systolic forward flow causes a
uniform elevation in the mean left atrial pressure,
that is, high diastolic forward flow. A shortened
deceleration time for the diastolic pulmonary venous
velocity is a good indicator of high left atrial pressure,
or wedge pressure.
Substantial progress has been made in the estimation
and more accurate prediction of pressures. A tight,
linear correlation between the mitral deceleration
time and pulmonary vein diastolic deceleration time
has been shown in patients with myocardial infarction.
Supporting new data shows that deceleration of the
pulmonary venous diastolic flow is more accurate than
the pulmonary artery occlusion pressure in predicting
left atrial pressure, and is more accurate than catheter-derived
data using the occlusion technique.
|
PAGE
TOP
|
End Diastolic
Event with Atrial Contraction |
 |
| Figure
4. Representative patterns of the four grades
of diastolic dysfunction. |
| Click
to enlarge |
|
Work from Japan in the experimental dog model of
infarction shows that as LV compliance is reduced,
atrial contraction occurs as the LV pressure rapidly
increases and exceeds the left atrial pressure, resulting
in a very short duration of forward flow. Clinically,
this method has been shown to accurately predict end
diastolic pressure.
The severity of diastolic dysfunction and the level
of the mean left pressure can be understood by evaluating:
the elevation of the left atrial pressure, left ventricular
end diastolic pressure, mitral natural history distribution
of velocities, reduced forward flow and E prime velocity
as measured by tissue Doppler, pulmonary vein measures,
and diastolic dominance and slow flow, as noted in
the color flow propagation, including diastolic deceleration
time (Figure 4).
|
PAGE
TOP
|
Left Atrium
and Diastolic Dysfunction |
|
Left atrial volume mirrors diastolic dysfunction
of the left ventricle. In hypertrophic cardiomyopathy
the left atrium is markedly enlarged. Left atrium
size is a quick indicator of the degree of diastolic
dysfunction in the absence of intrinsic mitral valve
disease.
Studies at the cellular level in a single myocyte
with calcium overload showed no difference in the
resting state between the wild-type and genetic knockout
mice. Beta adrenergic stimulation with isoproterenol
showed no diastolic overloading in the wild-type normal
myocyte. In contrast, in the diseased myocyte, beta
adrenergic stimulation caused progressively increased
diastolic loading, that is, diastolic dysfunction
is unmasked.
Relaxation abnormalities can now be investigated
in the cardiac catheterization and echocardiographic
laboratories, based on data obtained at the cellular
level. At Mayo Clinic in the echocardiography laboratory,
patients with baseline normal diastolic function and
only mild abnormalities are subjected to a bicycle
stress test. It is no longer sufficient to perform
only a Doppler examination in the resting state. The
next step of a stress test must be taken to non-invasively
unmask abnormalities.
|
PAGE
TOP
|
| Mortality and outcomes are similar for both forms
of heart failure. Data from the Mayo Clinic show that
the survival curve for both diastolic and systolic heart
failure is identical at up to four years of follow-up,
and is markedly lower than the expected survival of
the control population.
Outcomes can be stratified based on pulmonary artery
wedge pressure, as noted by Warner Stevenson at Brigham
& Women's Hospital in Boston. One-year survival
was excellent if the initial wedge pressure was little
elevated. Survival was intermediate if the initial
elevated wedge pressure was reduced to less than 16
mm Hg with treatment. Survival was poor if the pressure
remained elevated despite optimal medical treatment.
Since the Doppler provides insight into pulmonary
artery capillary wedge pressure, or mean left atrial
pressure, it is intuitive that the grade of diastolic
dysfunction will also inform about prognosis. Studies
at Mayo Clinic showed the worst survival in patients
with cardiac amyloidosis and severe diastolic dysfunction.
Dilated cardiomyopathy also has a poor prognosis.
In patients with dilated cardiomyopathy with an identical
ejection fraction, the survival was worse for those
with deceleration, which was markedly shortened, that
is, advanced diastolic dysfunction.
Simple mitral deceleration time can predict the outcome
for patients with ischemic cardiomyopathy. A markedly
shortened deceleration time indicates very few viable
segments and a high level of scarring. Post-operatively,
the least improvement in ejection fraction was predictive
and seen in patients with markedly shortened deceleration
time. The data is very similar to dobutamine echo
prediction. Profound insight into the management and
outcome of ischemic cardiomyopathy can be gained using
diastolic parameters, such as deceleration time. In
patients with acute myocardial infarction, restricted
ventricular filling is prognostic. Outcomes worsen
as the degree of diastolic dysfunction worsens.
A multicenter study of Doppler tissue imaging and
color flow propagation velocities concluded that advanced
diastolic dysfunction is associated with a worse prognosis.
A Doppler tissue imaging ratio greater than 10 indicated
a worse prognosis.
Italian investigators showed in patients with severe
diastolic dysfunction with shortened deceleration
time that outcomes were worse in the patients in whom
the deceleration time remained shortened despite optimal
medical treatment. Outcomes (survival, transplantation,
repeat hospitalization) improved in patients whose
deceleration time increased with treatment.
|
PAGE
TOP
|
|
Unlike the situation for SHF, no evidence-based treatments
are available for DHF, since there is no published
clinical trial evidence for treatment. However, multiple
trials are underway and results will become available
to provide the needed data. Until then, the emphasis
must be preventive measures, including optimal treatment
of hypertension, elimination of ischemia via interventions,
catheter-based or surgery, as with ischemic cardiomyopathy;
regression of hypertrophy, and reduction of calcium
overload and fibrosis.
The effective treatment of hypertension reduces
CHF incidence by 50%. However, the control of hypertension
is poor worldwide. In the United States, only 27%
of patients with hypertension are controlled to levels
less than 140/90mm Hg. In England, only 6% of patients
are controlled. The AT1 blocker losartan reduces the
development of heart failure, and improves the symptoms
of patients with heart failure.
Doppler profiles are useful to guide treatment.
In Grade One diastolic dysfunction, diuresis need
not be increased. The emphasis is to maintain synchrony,
reduce the heart rate to allow more time for diastolic
filling and maximize neurohumoral antagonism. Grade
One patients have the best prognosis. In contrast,
in Grade Three or Grade Four diastolic dysfunction,
there is marked elevation of filling pressures and
diuresis is needed under very controlled conditions.
Maximum neurohumoral antagonism is needed and the
patients must be followed very closely. These patients
have a poor prognosis, and if appropriate early consideration
for transplantation is needed.
|
PAGE
TOP
|
|
Investigators from Boston showed that in the adult
rat heart adenoviral gene transfer of sarcoplasmic
reticulum Ca2+-ATPase (AdSERCA2a) restored
diastolic dysfunction. With age, LV end diastolic
pressure increases. Gene therapy with AdSERCA2a resulted
in significantly lower end diastolic pressures that
were closer to normal. Also with age, relaxation slows,
but is returned to baseline levels with gene therapy.
A comparison of patients with classic hypertrophic
cardiomyopathy (gene positive, LVH present) and gene-positive
relatives without LVH (normal wall thickness) showed
that even in the presence of normal morphology the
latter group had abnormal Doppler tissue imaging.
Doppler tissue imaging detects abnormalities in the
actin myosin interaction at the molecular level. The
finding of a non-invasive measure of LV function using
Doppler tissue imaging that potentially predicts hypertrophic
gene positivity before the development of hypertrophy,
if substantiated by other investigators, will truly
revolutionize the understanding and management of
hypertrophic cardiomyopathy.
|
PAGE
TOP
|
|
A 10% incidence of atrial fibrillation (AF) was shown
in a study of 840 patients aged 75 to 100 years in
Olmstead County, with a mean follow-up of four years.
The development of AF could be predicted based on
the size of the left atrium. A low incidence of AF
was seen in patients with a low left atrial volume
index, while there was a high incidence of AF in patients
with a significantly elevated left atrial volume index.
The left atrial digitation correlated with the Doppler
finding. In patients with a normal pattern there was
no incidence of AF at 5 years. For patients with Grade
One or Grade Two dysfunction and abnormal relaxation,
the risk of AF was intermediate. The highest incidence
of AF was seen in the patients with Grade Three dysfunction
and a restrictive pattern. This now provides a non-invasive
marker to predict the patients at highest risk of
developing AF. Diastolic dysfunction appears to be
an important precursor of non-valvular AF in the elderly
population, with an independent, graded relationship
between the severity of diastolic dysfunction and
the risk of non-valvular AF.
|
PAGE
TOP
|
Report
Index | Previous Report
| Next Report
Scientific
Sessions | Activities
| Publications
Index
Copyright © 2002
Japanese Circulation Society
All Rights Reserved.
webmaster@j-circ.or.jp
|