|
|
||||||
|
|||||||
|
|||||||
|
|||
|
|||
History and Present Status of Takotsubo DiseaseSatoshi KurisuHiroshima City Hospital, Hiroshima, JapanTakotsubo disease (TD) was first reported in 1990 and now is accepted worldwide as a distinct clinical entity. TD should be considered in the differential diagnosis of anterior myocardial infarction (AMI), especially in elderly women. Although the prognosis for TD is favorable, it can cause various complications especially during the early phase. The first report of TD was by Sato and colleagues in 1990 in a Japanese journal where they reviewed five cases of takotsubo cardiomyopathy and suggested that it may result from stunned myocardium due to multivessel coronary spasm. In TD, left ventriculography and coronary angiography will not reveal any coronary artery disease (CAD), as they would in anterior AMI. Anteroapical wall motion is depressed in both TD and AMI, and ST-segments in precordial leads are often elevated in both disorders. Echocardiographic and electrocardiographic findings are similar in TD and AMI. The treatment for TD and AMI are different requiring early differential diagnosis.
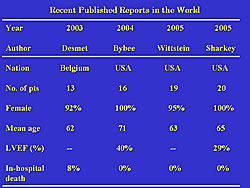
In 2000, Kawai and colleagues published an English-language paper on TD in the Japanese Circulation Journal, and thereafter it was accepted worldwide as a distinct clinical entity. Four reports of TD outside of Japan have been published, three from the United States and one from Belgium. Although the numbers are small, 92% or more of the patients were elderly women (Figure 1). From 1983 to 2005, there have been 65 patients (57 women) with TD at the Hiroshima City Hospital. The mean age was 73 years, 8 patients had diabetes, and 24 patients had hypertension. Acute left ventricular (LV) ejection fraction (LVEF) was 48%. TD is well known to be associated with mental stress, and in their patients its occurrence was associated with the death of a brother, syncope in husband, automobile accident of husband, and quarrel with husband. In our patients we found epileptic convulsion, tooth extraction, and dyspnea from bronchial asthma and serious pneumonia to physical stress triggers for TD.
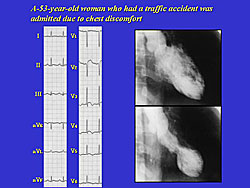
In a typical TD case associated with mental stress, a 53-year-old woman who had a traffic accident without trauma was admitted for chest discomfort. Her electrocardiogram showed ST elevation in precordial leads and ventriculography showed apical akinesia with no CAD (Figure 2). In a typical case of TD associated with physical stress, a 77-year-old man who underwent gastrointestinal examination was admitted due for chest discomfort. No gastrointestinal disease was found. His electrocardiogram showed ST elevation in precordial leads and the left ventriculography showed apical akinesia with no CAD. Several possible mechanisms have been proposed, including multivessel epicardial coronary spasm, microvascular coronary spasm, and catecholamine-mediated toxicity. The striking predominance of women suggests that sex hormones may exert important influences on the occurrence of TD.
Akinesia from the mid to distal portion of the left ventricle is the most impressive characteristic of TD. The apical ballooning can vary in size, and it is unclear what regulates the size of this ballooning (Figure 3). Another notable characteristic of TD is the resolution of LV asynergy within about 3 weeks, with, for example, LVEF at 42% at admission, 50% at day 7, and at 73% at 21 days. A typical time course of electrocardiogram shows that the ST elevation or T wave inversion is often observed during the early phase (Figure 4). ST elevation is observed especially in the right precordial leads. T wave inversion deepens progressively to its first negative peak, which occurs at about 3 days. The T wave is shallow for several days and then deepens again, the second negative peak occurring at approximately 2 weeks. The QT interval is prolonged as the T wave deepens, and shortened as the T wave becomes shallow. Kurisu reported that their in-hospital mortality was 5%, which is similar to that in other groups. Three patients died of pneumonia, renal failure or lung cancer, while no deaths resulted from TD itself. Although the prognosis is favorable, TD causes LV dysfunction during the early phase and can cause various subsequent complications. One complication seen at Hiroshima City hospital was two cases of LV apical thrombus formation, which led to a transient cerebral ischemic attack in one patient. This complication is also reported by other groups. To prevent thromboembolism, anticoagulant therapy should be given during the early phase. LV outflow tract obstruction was seen in 8 of the 65 patients at Hiroshima City Hospital. In a representative case, the pressure gradient was 74 mmHg between the LV apex and aorta.
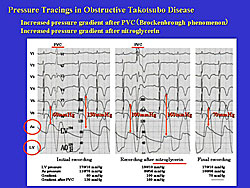
In a case of obstructive TD, left ventricular and aortic pressure tracings showed a peak systolic gradient of 60 mmHg in the initial recordings (Figure 5). On the first sinus beat after a premature ventricular contraction, the peak systolic gradient augmented to 130 mmHg, and the pulse pressure decreased. This is well known in hypertrophic obstructive cardiomyopathy and called Brockenbrough phenomenon. Shortly after intravenous administration of nitroglycerin, the recording showed that central aortic pressure decreased and the peak systolic gradient increased to 100 mmHg. Positive inotropic agents and nitroglycerin are often used to treat heart failure. However, these agents can augment the gradient. LV outflow obstruction should be assessed during early phase of TD. Malignant arrhythmia, especially torsade de pointes, was another complication seen by this group. A 2-fold increase in the prolongation of the QT interval is seen during the recovery phase in TD. In patients with TD, bradycardia or hypokalemia is often associated with QT interval prolongation and torsades de pointes may occur. Other reported complications include cardiac tamponade, left ventricular free wall rupture, and ventricular septal perforation. These complications are directly connected with sudden death and thus require early diagnosis and treatment. |

Clinical Characteristics of Takotsubo DiseaseYoshihiro AkashiSt. Marianna University School of Medicine, Kawasaki, JapanTakotsubo disease (TD) is thought to occur predominantly in elderly women, and their symptoms and some clinical findings resemble acute coronary syndrome. Reversible ventricular dysfunction in the apical area of the left ventricle (LV) is often seen. TD is sometimes referred to as ampulla cardiomyopathy, takotsubo transient ventricular dysfunction, apical ballooning, and stress-cardiomyopathy. Possible mechanisms of TD include physical or mental stress, autonomic dysfunction such as sympathetic nervous system hyperreactivity and dysregulation, factors at the myocardial or systemic level, genetic factors, and age. Regarding stress as a trigger, animal experiments have shown that stress in the cortex and limbic system may activate c-fos, a nervous excitation marker. A signal is transmitted to the hypothalamus, and spinal cord catecholamines are released. Autonomic dysfunction occurs, which can affect the heart and lead to various alterations and to adrenoceptor hyperreactivity and microvascular spasm. Systemically, autonomic dysfunction can accelerate secretion of norepinephrine, noradrenalin, or cytokines, perhaps leading to changes in the ion channel in the myocardium and perhaps myocardial injury. These processes may lead to TD, a reversible ventricular dysfunction. Akashi reviewed studies by his group including data that support the hypothesis that TD may be due to neurogenic stunned myocardium caused by acute cardiac autonomic dysfunction. Akashi and colleagues showed that plasma BNP concentration positively correlated with the left ventricular end-diastolic pressure (LVEDP) and delta-base value (difference between the diameter of the LVEDP and LV end-systolic pressure at 1 cm below the aortic valve). No correlations between BNP concentration and LV parameters were found. Hence, it seems that basal hypercontraction in the acute phase of TD may accelerate BNP production. A case presentation published in the literature revealed the highest levels of BNP concentration in TD was 1 day after hospital admission, and the secretion pattern was similar to that in acute myocardial infarction (AMI). The etiology of TD is unclear, but hypotheses about its onset include coronary vasospasm, microcirculation insufficiency, transient coronary occlusion, and elevated catecholamine levels. Animal experiments conducted by Ueyama and colleagues suggested that a change of adrenoceptor sensitivity in the myocardium may be a major cause of TD. Akashi and colleagues hypothesized that TD is a neurogenic myocardial disease. They conducted a study using MIBG myocardial scintigraphy to assess cardiac adrenergic innervation in patients with TD. Myocardial scintigraphy with iodine-123, meta-iodo-benzyl-guanidine (MIBG) was performed in the acute phase within 3 days of hospitalization and 3 months after hospital discharge. Anterior and lateral chest images were acquired before SPECT acquisition. Decreased myocardial perfusion at the distal anterior wall, the apex, and the inferior wall were found in the early acute phase SPECT images. Increased MIBG washout was seen on the 4-hour delayed images, and the chronic phase of early MIBG SPECT images showed still decreased MIBG uptake in the infero-posterior wall and apex. At 3 months, MIBG washout was less prominent. Remarkable cardiac adrenergic nervous dysfunction was present in the acute phase, whereas at 3 months there was a gradual improvement of myocardial adrenergic function. In the acute phase, the H/M ratio decreased significantly from 2.10 to 1.89, whereas in the chronic phase the H/M ratio did not decrease between the early and delayed image and the delayed H/M improved significantly from 1.89 to 2.10 through about 3 months. Cardiac sympathetic activity was remarkably elevated in an acute phase of TD, as shown by the accelerated global washout rate of MIBG in the acute phase, which significantly decreased and normalized from 43.3% to 29.5% at 3 months. Work by Akashi and colleagues showed that decreased heart rate variability in TD patients may reflect damage of the cardiac autonomic function. Akashi and colleagues evaluated cardiac autonomic function in 10 patients with TD and age-matched control subjects who suffered from stress in their daily life. The diagnostic criteria for TD were sudden heart failure with AMI-like symptoms, takotsubo-shaped hypokinetic LV revealed by LVG, and the absence of coronary artery disease on CAG. Holter monitoring was recorded after hospital admission and at 3 months in TD patients and during life in control subjects. Heart rate (HR) variability was analyzed using SCM-6000. The initial ejection fraction (EF) was 45.7%. The LV wall motion completely normalized within about 3 weeks and EF increased significantly to 69.8% (p<0.001). HR and mean NN interval in the acute or chronic phases did not differ significantly between the TD patients and the control group. Time domain analysis showed that SDNN and SDANN improved significantly in the chronic phase of TD after decreasing significantly in the acute phase. |
Takotsubo Cardiomyopathy Outside JapanMartin BorgreffeUniversity Hospital Mannheim, Mannheim, GermanyTakotsubo cardiomyopathy (TC) is now an accepted entity worldwide, not specific to Japan. TC can be regarded as a primary acquired cardiomyopathy, according to the recent classification of cardiomyopathies from the American Heart Association. Dr. Martin Borgreffe, University Hospital Mannheim, reviewed the characteristics of TC, the role of right ventricular (RV) dysfunction in TC, a presentation that is increasing, and TC in the setting of coronary artery disease (CAD).
Characteristics of TC The incidence of TC is unclear, occurring in 1-2% of patients with a suspected acute myocardial infarction (AMI) in Japan. In Europe, the incidence ranges from 0.07% of 5876 patients with ST-elevation MI in the Czech Republic to 2.5% of 2031 patients with suspected acute coronary syndromes (ACS) in Germany. The prevalence is higher in women (88% in Japan, 85% in Mannheim) and in the elderly (69 years in women and 66 years in women in Japan; 67 years in women and 74 years in men in Mannheim). Other characteristics are shown in Table 1.
Rare manifestations that occurred in the Mannheim series of patients included cardiogenic shock in 6%, syncope and left ventricular (LV) thrombus in 4%, and a 2% occurrence of recurrent monomorphic ventricular tachycardia and ventricular fibrillation.
Classical presentation: Left ventricular involvement Initial experience with TC primarily has involved the LV apex, which led to the term apical ballooning syndrome, based on the Japanese literature. Variants include classical, mid-ventricular, and basal, and other forms must be considered in TC. The mid-ventricular variant spares the LV apex. A reverse variant involves contraction of the apical region but ballooning of the base of the heart. However, Borgreffe stated that differentiation of these variants may not be justified because there seems to be a smooth transition from classical to variant TC. Further, he stated, spasm is over-emphasized and is a rare event worldwide, and myocardial dysfunction unrelated to the coronary tree is not seen. Therefore, this must be incorporated into the classical definition of TC.
Non-classical presentation: Right ventricular involvement Variants of TC not involving the LV apex are increasingly reported. In the Mannheim experience, 25% of patients had a non-classical presentation. The impressive LV dysfunction may have diverted attention from the right ventricle to date, stated Borgreffe, along with the difficulty of echocardiographic assessment of the RV and the obscure clinical significance of RV involvement. In a series of 51 patients with classical TC at University Hospital Mannheim, 47 underwent gadolinium-enhanced cardiac magnetic resonance imaging (CMR; 4 exclusions because of claustrophobia, metal implant). Of these, 34 patients had significant LV wall motion abnormality (WMA). To determine RV involvement and the presence of pleural effusion, the CMR studies were retrospectively reviewed by two independent investigators, who assessed the RV chamber using an 8-segment model. WMA was classified as hypokinesia, akinesia, or dyskinesia, and pleural effusion was visually estimated and classified as absent, mild (< 2 cm), or significant (> 2 cm). A total of 34 patients (32 women, mean age > 70 years) had RV involvement. RV WMA was identified in 9 (26%), whose presenting symptoms were angina (5 patients), dyspnea (3), and nausea (1). The peak CK was not dramatically high (ranging from 66-479 U/l) and LV ejection fraction ranged from 30-49%. RV dysfunction seems to be associated with more severely impaired LV function. Notably, 70% of patients presenting with TC and RV involvement had pleural effusion. Thus, the clinical diagnosis can be made at the bedside, especially if the pleural effusions are bilateral or significant, or a global ischemic event on ECG, in the presence of a typical TC acute ST-segment presentation.
TC and coronary artery disease The vast majority of past studies of TC have excluded patients with CAD. However, TC and CAD may coincide, so this may not be justified. TC and a non-critical lesion of the left anterior descending (diameter stenosis on QCA > 50 and <75) was the final diagnosis in 4 patients in a series of 821 consecutive patients seen by Borgreffe and colleagues from December 2004 and August 2006. All patients underwent urgent left heart catheterization for suspected acute coronary syndrome ACS. Notably, 2 of these 4 patients had a previous (6-8 months) coronary angiogram with no progression of CAD, and 2 of these 4 patients had IVUS which did show any plaque rupture, thrombus, positive remodeling, or intimal dissection. Borgreffe stated that excluding the diagnosis of TC on the sole basis of an incidental finding of CAD may not be justified in all cases. A case-by-case decision process seems more appropriate, balancing the clinical presentation, electrogram results, and the degree of LV and RV involvement. An analogy is a case of dilated cardiomyopathy with a 60% right coronary lesion where the extent of myocardial dysfunction is not explained by the non-critical right coronary lesion. No convincing evidence that plaque rupture plays a pathogenic role was found in this series. |
|
|
|
Copyright © 2007 Japanese Circulation Society All Rights Reserved. webmaster@j-circ.or.jp |