The importance of this phenomenon is to
ascertain whether or not preconditioning occurs in humans.
Pre-infarct angina or directly inducing angina (warm-up
angina) could be considered as naturally-occurring forms
of preconditioning in humans. In this regard, numerous
studies using retrospective analyses (in the thrombolytic
era) show that pre-infarct angina provides a better overall
clinical outcome. An example of this is the TIMI-4 which
showed that patients with pre-infarct angina had a better
overall clinical outcome.
Other examples of potential pre-conditioning
in patients is in the setting of warm up angina. Warm
up angina describes the ability of some patients to exercise
to angina, rest, and then continue exertion with few or
no symptoms. Clinical analogies include "walk through
angina" and "second wind angina." A number of studies
show that on the second exercise test there is improved
exercise duration, decreased ST segment depression, decreased
ischemic threshold, and decreased mVO2; all
beneficial outcomes implying that preconditioning in humans.
However, these do not directly prove the existence of
human preconditioning.
|
PAGE
TOP
Studies
to determine the existence of human preconditioning |
|
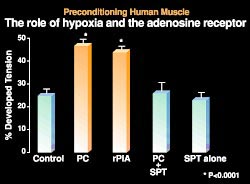 |
Figure
1. Human muscle subjected to 90 minutes of hypoxia
and 2 hours of re-oxygenation had a 25% functional
recovery (control). Muscle subjected to a 3-minute
hypoxic insult and 7 minutes of re-oxygenation
prior to the 90-minute insult had a significantly
improved functional recovery (PC). CCPA, an adenosine
analogue used in place of hypoxia, produced protection
similar to that with preconditioning (rPIA). The
protective effect of preconditioning was abolished
in the presence of SPT (PC and SPT) and the adenosine
receptor antagonist. SPT alone had no effect (SPT).
(J Moll Cell Cardiol 1995;27;1349-1357.)
Click
to enlarge |
|
Studies were undertaken by Yellon's
laboratory to determine whether human muscle can
be pre-conditioned and whether there is a role for
the adenosine receptor. Atrial muscle from human
right atrial appendage of patients undergoing cardiac
bypass surgery was placed in an organ bath. The
trabeculae were attached to a fixed post and the
other end to a force transducer to measure functional
recovery. The human muscle was directly subjected
to a preconditioning protocol of 3 minutes of hypoxia
and 7 minutes of re-oxygenation prior to a lethal
ischemic insult of 90 minutes.
Human muscle preconditioning and
a role for the adenosine receptor were shown in
their first study (Fig. 1). Human muscle subjected
to 90 minutes of hypoxia and 2 hours of re-oxygenation
had a 25% functional recovery. But, 48% functional
recovery was obtained when muscle was subjected
to a 3-minute hypoxic insult and 7 minutes of re-oxygenation
prior to the 90-minute insult. CCPA, an adenosine
analogue used in place of hypoxia, produced protection
similar to that with preconditioning. In addition,
the protective effect of preconditioning was abolished
in the presence of SPT, the adenosine receptor antagonist.
SPT alone had no effect.
|
|
PAGE
TOP
Potential
signalling pathways |
|
 |
|
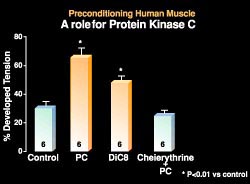
Figure
2. The PKC inhibitor chelerythine was given
to determine whether any observed effect can
be abolished. In addition, DiC8, a PKC analogue,
was given to stimulate protein kinase C. (Circ
Res 1995;77:1030-1035.)
Click
to enlarge
|
|
Similar signalling pathways to that
seen in the experimental models were seen in studies
in Yellon's laboratory focusing on protein kinase
C (PKC). The PKC inhibitor chelerythine was given
to ascertain whether any observed effect can be
abolished. In addition, DiC8, a PKC analogue, was
given to stimulate PKC. In human muscle, 30% functional
recovery was regained after 90 minutes of hypoxia
and 2 hours of re-oxygenation in the control (Fig.
2). About a 70% functional recovery was regained
after preconditioning with 3 minutes of hypoxia
and 7 minutes of re-oxygenation. When DiC8 was substituted
for preconditioning to activate PKC about 50% functional
recovery was obtained. The protective effect was
abolished with chelerythine.
|
|
PAGE
TOP
KATP
channel is a preconditioning end-effector |
|
KATP involvement was
shown in studies using the KATP channel
opener cromakaline and the KATP channel
blocker glibenclamide. The human muscle control
had about a 30% functional recovery. With preconditioning,
used as a positive control, there was approximately
a 60% recovery of function. A similar effect was
obtained with the KATP channel opener
cromakaline. However, the effect of preconditioning
as well as the effect of cromakaline was abolished
when given in conjunction with the KATP
channel blocker glibenclamide. Glibenclamide alone
had no effect.
That KATP was shown
to be downstream of PKC was observed when DiC8 was
given to activate PKC and this was blocked by the
KATP channel blocker. Preconditioning
and cromakaline provided good functional recovery,
about 62% and 58%, respectively. DiC8 alone provided
functional recovery of about 50%. However, the protective
effect was abolished with DiC8 was given in the
presence of glibenclamide.
|
|
PAGE
TOP
Other
therapeutic options |
|
Opioid receptors have also been shown
to play a role in triggering preconditioning in
animal hearts. A number of receptors, including
the mu, delta, and kappa, exist in the heart. The
distribution of opioid receptors in the human heart
favors the mu and delta subtypes. Using human atrial
and ventricle muscle Yellon's group was able to
show that in both muscles the mu and delta receptors
were expressed abundantly, compared to the kappa
receptor.
The opioid receptor was shown to
be a preconditioning trigger in human atrial muscle.
Again hypoxic preconditioning provided significant
protection with about a 43% functional recovery,
compared to 28% in control (p<0.001). The protective
effect of preconditioning was abolished when preconditioning
in the presence of naltrindole, a delta opioid receptor
antagonist. Naltrindole alone had no effect. DADLE,
a delta opioid receptor agonist, given alone provided
protection similar to that seen with hypoxic preconditioning
(p<0.001 vs control). Furthermore, hypoxic preconditioning
with 5-HD (the mitochondrial KATP channel
blocker) or DADLE with 5-HD abolishes the protective
effect, indicating that the mKATP is
involved in preconditioning using the opioid receptor
agonist.
|
|
PAGE
TOP
|
| |
Studies in low risk patients undergoing
coronary artery bypass grafting (CABG) was done
by Yellon's group to determine whether patients
undergoing CABG needed additional myocardial protection
and, if so, whether preconditioning can be of any
benefit either prior to, or during, bypass surgery.
Cardioplegia and cross clamp fibrillation are used
to protect the myocardium during CABG. However,
there are problems with both. Cardioplegia is not
uniformly distributed and the time of cross clamp
fibrillation is limited. Both techniques also involve
whole body cooling.
Patients were randomized to preconditioning
(n=17) or control (n=16) groups. The preconditioning
group received 3 minutes of cross clamping of the
aorta followed by 2 minutes of reperfusion followed
by another 3 minutes of cross clamping. The control
patients did not receive this preconditioning stimulus.
All patients then underwent 3 separate periods of
cross clamp fibrillation (10 minutes) during which
the graft was sown on.
|
 |
|
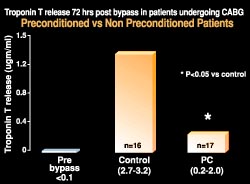
Figure
3. Patients undergoing coronary bypass surgery
randomized to the control group had significantly
greater troponin T levels than those in the
preconditioning group (PC). Troponin T was used
to measure tissue necrosis. (Heart 1997;77:314-318.,
with permission from the BMJ Publishing Group)
Click
to enlarge
|
|
Troponin T was used to measure tissue
necrosis; blood samples were examined after 72 hours.
The patients in the control group had significantly
greater troponin T levels compared to the preconditioning
group (about 1.4 µgm/ml vs about 0.2 µgm/ml;
p<0.05) (Fig. 3). This study provided proof of
concept that preconditioning in patients undergoing
CABG results in a direct benefit in terms of less
troponin T.
To evaluate the effects of adenosine
in preconditioning before bypass surgery, a blinded
randomized study using an experimental adenosine
A1 receptor agonist (GR79236x) was performed.
Patients were randomized to four groups (10 per
group): control, cold cardioplegia, preconditioning
(2 x 3-minute bursts of ischemia, each followed
by reperfusion), and an adenosine A1
receptor agonist (given over 10 minutes followed
by wash out).
There was an indication that the adenosine
A1 receptor agonist was having some beneficial
effect. The level of troponin T release was similar
to that in the preconditioning group, although this
did not reach statistical significance. Whether
the study was underpowered is unclear. In the control
group, there was a significant increase in troponin
T compared to the preconditioning group, showing
again preconditioning confers protection by reducing
troponin T release. The troponin release was similar
in the cardioplegia and control groups.
|
|
PAGE
TOP
|
|
Preconditioning is a form of cellular
adaptation that is highly protective. It has multiple
triggers, a complex signalling pathway, and speculative
end-effectors. Preconditioning occurs in the clinical
setting. From proposed mechanisms it may be possible
to design appropriate pharmacology for therapeutic
exploitation.
|
|
PAGE
TOP
Report
Index | Previous Report
| Next Report
Scientific
Sessions | Activities
| Publications
Index
Copyright © 2000
Japanese Circulation Society
All Rights Reserved.
webmaster@j-circ.or.jp
|