|
|
|
|
| Current and Future Perspectives of Minimally Invasive Cardiovascular Surgery |
|
|
|
|
|
Outcome of Off-Pump CABG and the Future Perspectives. Results of Off-Pump CABG in 694 patients since 1993.
Hirofumi Takemura
Kanazawa University Graduate School of Medical Sciences, Kanazawa, Japan
|
 |
| Figure
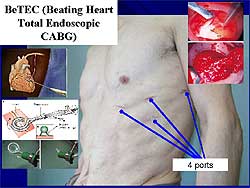
1. Beating heart total endoscopic CABG uses only
4 small keyholes to harvest the mammary artery
and anastomose the left anterior descending artery. |
| Click
to enlarge |
 |
| Figure
2. Only 3 or 4 small skin incisions from the groin
to the knee are needed to remove the saphenous
vein using the Mayo external vein stripper.
|
| Click
to enlarge |
|
Less invasive coronary artery bypass graft (CABG)
is defined most commonly as having a small skin incision
for the approach to the heart and for graft harvesting,
avoidance of the use of cardiopulmonary bypass (CPB),
or beating heart surgery with general anesthesia (OPCAB).
BeTEC (Beating heart total endoscopic CABG) was performed
in 6 patients. Through 4 small keyholes, the mammary
artery is harvested and the anastomosis of the left
anterior descending artery is performed (Figure
1). A newly developed heart stabilizer facilitated
this operation. After insertion into the thorax it
curls itself up inside the thorax to transform into
a circular heart stabilizer.
In one patient who underwent a MIDCAB, a skin incision
of only 3 cm was needed because the ITA was harvested
endoscopically. Another technique for LITA-LAD anastomsis
is a lower partial sternotomy incision, with the anastomsis
performed similarly to that in a full sternotomy operation.
The Mayo external vein stripper, a long metal bar
with a small circle on the tip, is one technique for
graft harvesting. It is inserted through a small groin
incision and the large saphenous vein exposed and
cut off. The vein stripper is slipped around the vein
and a small incision made if resistance is felt. The
vein is pulled out and branches detected and cut off.
After taking the full length of the vein, the branches
are clipped. Usually only 3 or 4 small skin incisions
are sufficient to remove the saphenous vein from the
groin down to the knee (Figure
2). This technique requires only about 15 minutes,
about the same time required for standard skin incision
technique. This group is working on removing the radial
artery endoscopically.
|
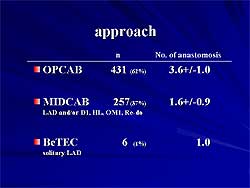 |
| Figure
3. The types of off-pump procedures used from
1993 to 2003 in 694 patients. |
| Click
to enlarge |
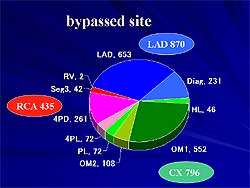 |
| Figure
4. The bypassed recipient arteries used in the
off-pump procedures. |
| Click
to enlarge |
|
Off-pump surgery
This group has performed OPCAB in 95% of
all patients in their hospital since 1993. Considerations
include graft selection, complete revascularization,
safety, and results. Between 1993 and 2003, they performed
OPCAB in 694 patients (553 male, 141 female, mean
age 66 years, range 37-91 years). The diagnosis was
old myocardial infarction in 525 patients, unstable
angina in 88, and stable angina in 81 patients. Co-morbidities
were CVA in 106 patients, difficult aorta in 88, chronic
renal failure in 35, COPD in 16, re-do surgery in
32 patients, and malignancy in 32 patients. The approach
used in these patients is shown in Figure
3.
The bypassed recipient arteries are shown in Figure
4. All coronary arteries were selected for target
site and could be bypassed equally. The complete revascularization
rate was 98.6% in the OPCAB patients and 90.4% in
the MIDCAB patients. The mean number of grafts was
3.4 in OPCAB patients and 1.6 in MIDCAB patients.
To ensure safety, this group uses the coronary active
perfusion system (CAPS), a mini extra-corporeal circulation
that consists of a small pump to push the blood into
the distal coronary artery during operation. CAPS
ensures a safer OPCAB and removes the need to rush
during anastomosis.
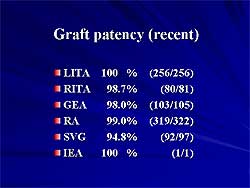
The graft patency rate is shown in Figure
5. The 30-day mortality was 1 death (0.14%) due
to incomplete revascularization. In-hospital mortality
was 1 death (0.14%), due to incomplete revascularization
in a re-do case. Morbidity was stroke (cerebral bleeding)
in 4 patients (0.5%), and exploration for bleeding
in 4 patients (0.5%).
OFCAB in these 694 patients had a low rate of mortality
and morbidity, a high rate of complete revascularization,
and a high rate of graft patency.
|
 |
| Figure
6. The degree of invasiveness of coronary artery
bypass surgery. The horizontal line represents
the degree of skin incision, the axis is the avoidance
of cardio-pulmonary bypass, and the vertical line
represents the use of intubation. |
| Click
to enlarge |
|
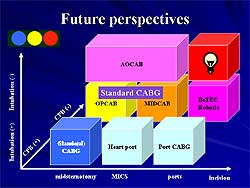
Future perspectives
Least-invasive CABG, including endoscopic
surgery, robotic surgery, hybrid OPCAB, and awake
OPCAB, is the current focus of this group.
Awake off-pump CABG (AOCAB) has been performed in
6 patients with LAD single-vessel disease. Three patients
received a GEA-LAD with a mid-abdominal incision;
1 patient had a LITA-LAD via MIDCAB; and 2 patients
had a full sternotomy with a LITA-LAD, LITA-LAD, and
branched RA-D1. No tracheal intubation was used, high
thoracic epidural anesthesia was used, and all patients
breathed spontaneously.
The degree of invasiveness of CABG as perceived by
this group is illustrated in Figure
6. Standard CABG with midsternotomy, CPB, and
intubation is becoming old-fashioned and its use is
decreasing. At their hospital, OPCAB and MIDCAB are
now the standard operation, and is used in 25% of
CABG patients, including acute cases. For the future,
approaches may be BeTEC, a hybrid procedure (PCI plus
CABG), awake OPCAB, and robotic surgery.
|
PAGE
TOP
|
Off-Pump
CABG: Hybrid Procedure and Robotic Surgery
Akimitsu Yamaguchi
Hayama Heart Center, Kanagawa,
Japan
|
|
Offpump coronary artery bypass surgery (OPCAB) has
gained worldwide interest as minimally invasive cardiac
surgery. The combination of percutaneous catheter
intervention (PCI) and coronary artery bypass, a so-called
hybrid procedure, can minimize the operative invasiveness.
This group has begun endoscopic atraumatic coronary
artery bypass (Endo A-CAB) using the AESOP endoscopic
system. This procedure can further minimize sternum
trauma or re-injury.
OPCAB was performed in 283 patients with a mean age
of 68 years (28% female) between 1996 and 2001. Pre-operative
coronary lesions were single vessel disease in 134
patients and multivessel disease in 149 patients.
The indications for OPCAB were CVA in 52 patients,
renal failure and heart disease in 36 patients, re-do
CABG in 24 patients, difficult aorta in 26 patients,
malignancy in 25 patients, peripheral vessel disease
in 18 patients, hemorrhagic concerns in 11 patients,
and cold in 18 patients. The remaining indications
were social reasons.
|
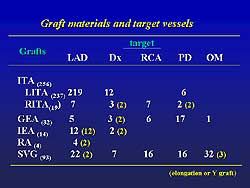 |
| Figure
1. The graft materials and target vessels used
in the off-pump procedures. |
| Click
to enlarge |
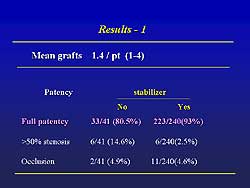 |
| Figure
2. The patency achieved and the use of a heart
stabilizer in the off-pump procedures.
|
| Click
to enlarge |
 |
| Figure
3. The operating room set-up for using the AESOP
endoscopic system. |
| Click
to enlarge |
|
The approach to the heart was full sternotomy in
161 patients, left thoracotomy in 91 patients (MIDACAB
in 87 patients), subxiphoid in 7 patients, and lower
half hemisternotomy in 24 patients. The graft materials
and target vessels are shown in Figure
1.
Of the 149 cases with multivessel disease, complete
revascularization was achieved with OPCAB in 82 patients
(55%). Hybrid therapy was performed in 41 patients
(27.5%), comprising a combination of OPCAB and PCI.
This was performed on the same day as OPCAB or within
7 days. The site of PCI was the right coronary artery
in 21 patients, left circumflex in 17 patients, diagonal
in 2 patients, and left main trunk in 5 patients.
The patency achieved and the use of a heart stabilizer
are shown in Figure
2. In-hospital death occurred in 5 patients (1.8%)
and late death in 6 patients (2.1%).
Based on the good results with the hybrid procedure,
they began using the Endo-A-CAB procedure, using endoscopic
left internal thoracic artery harvest and LITA-LAD
grafting through a small incision in the 4th intercostals
space. The set-up of the operating room is shown in
Figure
3. The AESOP endoscopic system is controlled by
the surgeon’s voice command. Three ports are
used for endoscopic LITA harvest. A port is placed
between the 3rd and 4th intercostals space for the
cautery, a port for the grasper through the 7th intercostal
space, and a port for the endoscope through the 5th
intercostal space. Anesthesia and single-lung ventilation
using a double-lumen endotracheal tube to permit collapsing
of the lung is performed. The patient is placed in
a semioblique position supported by an inflatable
pillow and is draped as for a conventional CABG procedure
The positioning of the patient is illustrated in Figure
4. When harvesting ITA using AESOP, the surgeon
holds the electric cautery in the right hand and the
grasper in the left hand. Voice commands spoken into
a microphone control the endoscope. This group has
performed endoscopic ITA harvest in 5 cases, as detailed
in Figure
5.
|
|
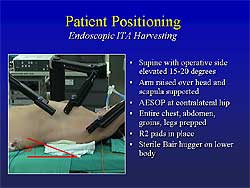 |
| Figure
4. The positioning of the patient for the AESOP
endoscopic procedure. |
| Click
to enlarge |
|
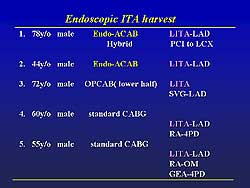 |
| Figure
5. The results of the endoscopic ITA harvesting
using the AESOP endoscopic system. |
| Click
to enlarge |
|
|
Comparison of Endo-ACAB and MIDCAB
Harvest of LITA requires a 6-8 cm incision between
the ribs, but the ACAB requires only tiny ports and
a 4 cm incision. In MIDCAB there is substantial horizontal
and vertical rib spreading, whereas there is none
for ACAB. In MIDCAB, often cartilage or a rib is removed,
which is not needed for ACAB. MIDCAB allows direct
visualization, loop magnification is used, lighting
is limited in the deep space, and a limited ITA length
can be harvested. In contrast, ACAB uses high-resolution
video, 10-15x magnification, excellent lighting from
the scope, the full length can be harvested from the
1st to the 6th intercostals space, and the entire
procedure can be recorded. With ACAB, the pericardium
can be opened and the target vessel located endoscopically
and the incision can be made directly over the target.
ABCAB also provides for easier checking of graft bleeding.
This group concludes that the Endo-ACAB procedure
and hybrid strategy can be used for multivessel disease.
The rationale for the hybrid strategy is that LAD
revascularization is the strongest predictor of prolonged
life. The LITA graft has better long-term results
than any other LAD therapy. Stenting results of other
vessels (non-LAD) are comparable with surgery.
The patient is the real winner. No cardiopulmonary
bypass is needed and complete revascularization is
achieved, with minimal pain, a good cosmetic result,
quick rehabilitation and return to work, and a good
long-term result.
|
|
Report
Index | Previous Report
| Next Report
Scientific
Sessions | Activities
| Publications
Index
Copyright © 2003
Japanese Circulation Society
All Rights Reserved.
webmaster@j-circ.or.jp
|
|